Angie – Registered Midwife of almost 14 years who wants positive change for women, people, their families and those who work in Maternity services. Midwives working conditions are women, people and their families pregnancy and birthing conditions.
Executive Summary
Safe staffing is fundamental to delivering high-quality maternity care. In England, however, there are currently no mandated national staffing standards for antenatal or postnatal inpatient maternity wards, despite clear evidence linking midwifery staffing levels to safer outcomes, improved patient experience, and workforce wellbeing. While intrapartum care benefits from a recommended one to one midwife to woman or person ratio during labour and birth, this prioritisation can inadvertently divert staff away from other areas of maternity services, such as antenatal and postnatal wards, community midwifery, and triage or assessment units. This imbalance contributes to delays in care, suspension of services such as home birth services or birthing centres, and increased pressure on the workforce.
At the same time, the financial and human consequences of unsafe maternity care are substantial. NHS maternity negligence claims account for £37.5 billion of the total clinical negligence provision, highlighting the urgency of addressing workforce models as a patient safety priority. The care hours required in maternity services has significantly increased due to increasing medicalisation of childbirth such as rising induction and caesarean section births, increasing maternal complexity and social deprivation, without the corresponding increases in workforce establishment.
This report examines the relationship between staffing levels and maternity safety, drawing on evidence from existing research and a Freedom of Information (FOI) request sent to 98 NHS Trusts out of 120 in England, with responses received from 50 Trusts. The FOI explored staffing models across antenatal, postnatal, and mixed maternity wards to identify national variation in patient-to-midwife ratios and workforce models.
The findings reveal substantial variation in staffing ratios across England, particularly in postnatal care. When only women were counted as patients, midwife-to-patient ratios on postnatal wards ranged from 1:4.5 to 1:10.3 during the day and 1:4.5 to 1:13 at night. Currently, babies are not counted as inpatients any Postnatal or mixed antenatal and postnatal maternity ward. When babies were included in the calculation, the number of individuals a single midwife could be responsible for increased dramatically, ranging from 9 to 26 women and babies per midwife overnight, with an Interquartile range of 13–16. This highlights a significant national oversight in workforce planning, given that newborns often require monitoring, feeding support, and clinical observations. This is a hidden understaffing ratio not being reported.
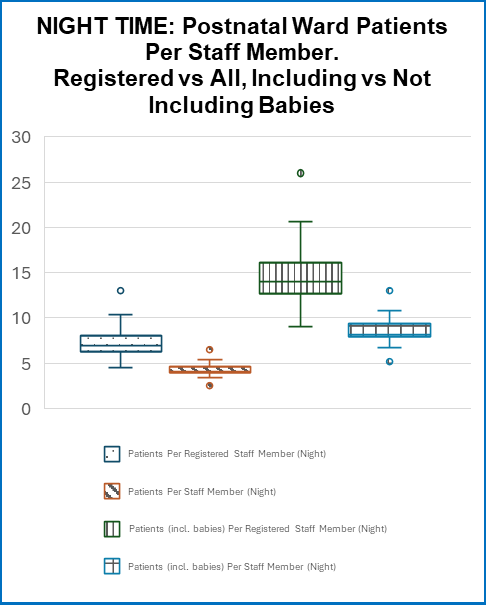
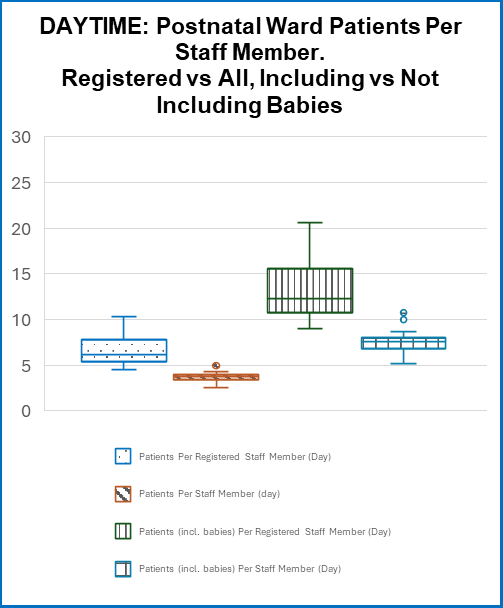
Antenatal wards demonstrated slightly lower ratios, typically 4.5–6.5 patients per midwife, although variation still existed. In mixed antenatal and postnatal wards, ratios ranged widely, reaching up to 21 women and babies per midwife at night in some units. Additionally, many Trusts reported reducing staffing overnight, particularly on postnatal wards, potentially increasing risks during periods already associated with higher healthcare mortality in other settings.
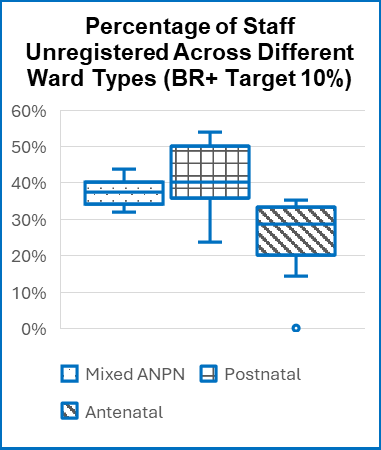
This report also highlights significant inconsistencies in skill mix. Although national guidance from Birthrate Plus (BR+) recommends a workforce of approximately 90% registered midwives and 10% maternity support workers, many units reported higher proportions of support staff within their daily staffing workforce. In some Trusts, there were more support workers on shift than registered midwives, raising concerns about the substitution of registered clinical expertise with unregistered staff despite limited evidence that such substitution improves clinical outcomes.
The use of Birthrate Plus (BR+) and other acuity tools also varies widely. While most Trusts rely on these tools to calculate staffing needs in intrapartum settings, evidence supporting their effectiveness remains limited, and their use outside intrapartum settings is relatively new. Compliance with completing ward acuity assessments was often low in the Trusts who did use this, and one Trust reported concerns about the accuracy or usability of the tool. Importantly, acuity tools do not currently capture workload in community services, maternity triage, or outpatient clinics, leaving significant gaps in workforce planning.
Evidence consistently demonstrates that midwifery understaffing is associated with increased harm. Studies show that lower midwifery staffing levels correlate with an 11% increase in reported harmful incidents, higher maternal readmission rates, poorer patient experience, and increased risk of missed care. Workforce pressures also affect staff wellbeing, with 45% of midwives reporting high levels of stress, and burnout cited as one of the leading reasons professionals leave the register. Midwives in England are estimated to work over 100,000 unpaid hours each week to maintain service provision.
This FOI findings further highlight inconsistencies in transitional care staffing for newborns requiring additional monitoring or treatment. Only half of Trusts counted babies as patients in these settings despite national recommendations from the British Association of Perinatal Medicine for one nurse or midwife to four babies.
Taken together, these findings demonstrate a significant lack of standardisation in maternity staffing across England, with wide variation between Trusts in daily staffing provision and the range of patients per Midwife, along with limited national oversight. The CQC can take enforcement action if organisations do not have enough suitably qualified staff. However, with many organisations not on a ward based acuity tool, nor looking at rotas nor acuity tool reports to see how regularly they are working in the red on low levels of staffing on a regular basis and outside of CQC inspections, how does this ensure oversight? Without clear minimum staffing standards, organisations are left to determine workforce models locally, CQC have no benchmark to compare against and this then leads to inequitable care provision which could have potential impacts on outcomes, experiences and safety.
This report therefore calls for nationally mandated staffing standards across all maternity inpatient settings, including antenatal and postnatal wards, alongside the inclusion of babies within patient ratios. Recommendations include establishing minimum ratios for postnatal and antenatal care, limiting the number of ongoing inductions a midwife can provide care for, systems to have oversight of acuity data, and reviewing workforce skill mix to ensure the appropriate balance between registered midwives and support staff.
Improving staffing levels is not only critical for reducing avoidable harm but also for improving patient experience, supporting workforce retention, and ensuring sustainable maternity services. Addressing these workforce challenges requires coordinated national leadership, robust data monitoring, and targeted investment to ensure that all women, birthing people, and babies receive safe and compassionate care across England’s maternity services.
For the full report in detail email theecomidwife@outlook.com
Safer staffing qualitative responses.
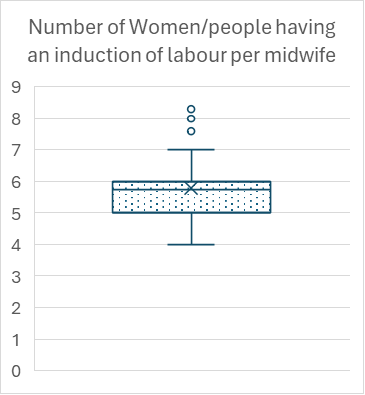
In total 16 Trusts responded to state they have frameworks to support safe staffing models in their Trust. However, only one Trust responded with the following template for safe staffing across maternity inpatient areas. In addition, two Trusts stated they have a recommendation of 1 midwife to 4 women or people having an induction of labour.
Many Trusts stated they use the BR+ tool to move staff on a shift-by-shift basis based on acuity. Trust A50 stated
‘We do not determine a ratio of staff to a number of beds. Staffing and establishments are determined by the BirthRate Plus staffing tool’.
This Trust only uses the intrapartum BR+ tool. Similar responses were received by three other Trusts who stated they monitor staffing on a shift-by-shift basis using BR+, but only use the Intrapartum tool. In reality these Trusts are only using escalation and acuity figures to guide the workforce required in intrapartum settings and not in other inpatient maternity ward areas. Highlighting the issues in mandating only one specific area of maternity services having specific staffing standards.
There were further inaccuracies or conflicting answers within some of the same responses with the safer staffing question. As an example, Trust A3 stated ‘The usual ratio is 1:8.’ This Trust then highlighted their daily staffing template ratio was each midwife caring for 9.25 patients on a daily workforce model basis due to the number of beds (not including babies – with babies this was 1:18.5).
Another comment from Trust A45 ‘Newborn babies on the postnatal ward are cared for by their mothers. Sick babies are cared for on the Neonatal unit. It does have to be acknowledged this was from a Trust with a higher number of midwives to patient ratio where the registered staff to patient ratio was 1 member of staff to 5.8 and including babies was 1 member of registered staff to 9.8 patients and babies. Analysis of whether babies requiring observations for blood sugar monitoring, intensive infant feeding support or two hourly observations was not explored as to whether these babies would meet the sick baby criteria in a neonatal unit, or alternatively on the postnatal ward. This comment was reflected in many other responses where ‘new mothers are expected to care for their baby’, regardless of mode of birth or care required themselves.
In relation to staffing and acuity, some Trusts had more innovative ways of working to ensure safer staffing implementation across maternity services. As an example, several Trusts implemented a ‘bed coordinator’ or ‘senior midwife’ to assess all inpatient and outpatient areas daily to facilitate the movement of staff where acuity was deemed higher than midwifery staffing hours. However, these were often during daytime hours and weekdays only it appeared in the Trusts who responded with this way of working.
